DESCRIPTION
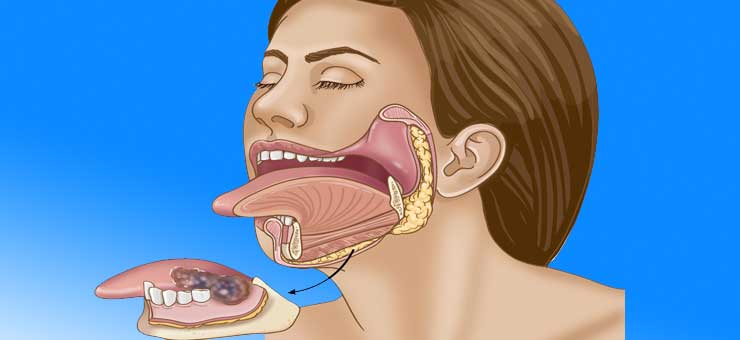
- Mouth cancer surgery, also known as mouth cancer, is a cancer of the lining of the lips, mouth, or upper throat.In the mouth, it most commonly starts as a painless white patch, that thickens, develops red patches, an ulcer, and continues to grow.
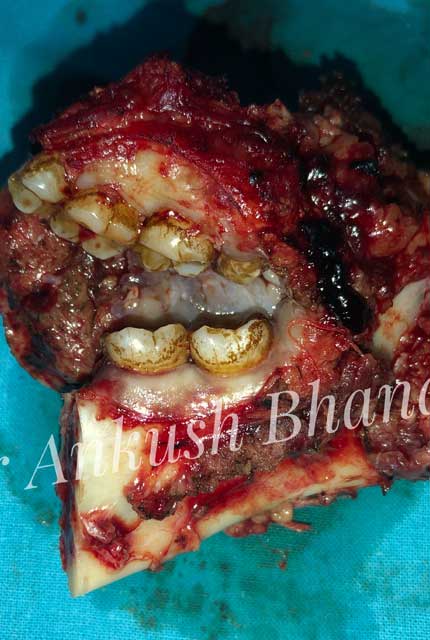
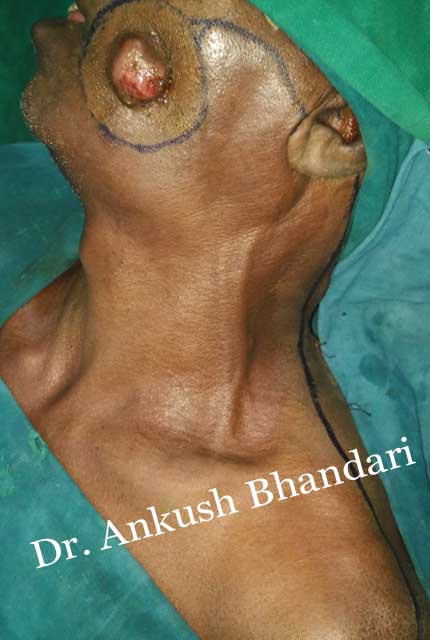
- In most centres, removal of squamous cell carcinoma from the oral cavity and Head & neck is achieved primarily through surgery. This also allows a detailed examination of the tissue for histopathologic characteristics, such as depth, and spread to lymph nodes that might require radiation or chemotherapy, access to the oral cavity is through the mouth. When the lesion is larger, involves the bone of the maxilla or mandible, or access is limited due to mouth opening, the upper or lower lip is split, and the cheek pulled back to give greater access to the mouth When the tumor involves the jaw bone, or when surgery or radiation will cause severe limited mouth opening, part of the bone is also removed with the tumor.
- Diagnosis of oral cancer surgery is completed for Initial Diagnosis, Staging, and Treatment Planning. A complete history, and clinical examination is first completed, then a wedge of tissue is cut from the suspicious lesion for tissue diagnosis. This might be done with scalpel biopsy, punch biopsy, fine or core needle biopsy. In this procedure, the surgeon cuts all, or a piece of tissue, to have it examined under a microscope by a pathologist. Brush biopsies are not considered accurate for the diagnosis of oral cancer surgery.
With the first biopsy, the pathologist will provide a tissue diagnosis , and classify the cell structure. After a histologic diagnosis has been established and tumor extent determined, the selection of appropriate treatment for a specific cancer depends on a complex array of variables, including tumor site, relative morbidity of various treatment options, concomitant health problems, social and logistic factors, previous primary tumors, and the person's preference. Treatment planning generally requires a multidisciplinary approach involving specialist surgeons and medical and radiation oncologists.Surgical resection and radiation therapy are the mainstays of treatment for most head and neck cancers and remain the standard of care in most cases.
For small primary cancers without regional metastases (stage I or II), wide surgical excision alone or curative radiation therapy alone is used. More extensive primary tumors, or those with regional metastases (stage III or IV), planned combinations of pre- or postoperative radiation and complete surgical excision are generally used. More recently, as historical survival and control rates are recognized as less than satisfactory, there has been an emphasis on the use of various induction or concomitant chemotherapy regimens.